Acupuncture And Herbs Beat Drug For Ankylosing Spondylitis
 Acupuncture and herbs outperform sulfasalazine for the alleviation of ankylosing spondylitis. Henan University of Traditional Chinese Medicine researchers investigated the benefits of drugs, acupuncture, and herbal medicine for the treatment of ankylosing spondylitis. The researchers conclude that acupuncture plus herbs is more effective than the sulfasalazine (an antirheumatic medication).
Acupuncture and herbs outperform sulfasalazine for the alleviation of ankylosing spondylitis. Henan University of Traditional Chinese Medicine researchers investigated the benefits of drugs, acupuncture, and herbal medicine for the treatment of ankylosing spondylitis. The researchers conclude that acupuncture plus herbs is more effective than the sulfasalazine (an antirheumatic medication).
Three groups were compared. One received only drug therapy. Another received herbal medicine. Another group received herbal medicine plus acupuncture. The group receiving herbal medicine plus acupuncture achieved the highest positive patient outcome rate of 52.8%, with only a 2.8% adverse effect rate. The drug therapy group had an adverse effect rate of 38.7%. In additional to clinical subjective improvements, the acupuncture plus herbs group achieved the greatest improvements in radiographic changes and levels of C3, ESR,CRP, and PHI. Primary outcome measures for the study included the following:
- Bath Ankylosing Spondylitis Patient Global Score (BAS-G)
- Bath Ankylosing Spondylitis Disease Activity Index (BASDAI)
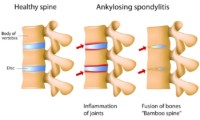
- Bath Ankylosing Spondylitis Radiology Index (BASRI)
- Bath Ankylosing Spondylitis Metrology Index (BASMI)
- TCM Syndrome Differentiation (TCM Symptom) Scale
BAS-G is a global measure used to assess the well-being of patients with ankylosing spondylitis. BASDAI is a diagnostic tool used to determine patient reported disease activity in patients with ankylosing spondylitis. BASRI is an objective method used to grade radiographic changes in AS (ankylosing spondylitis) patients. BASRI is an instrument used to quantify the mobility of the spine in AS patients. TCM (Traditional Chinese Medicine) symptom improvement was evaluated based on the TCM Syndrome Differentiation Scale.
Laboratory parameters were quantified, including the erythrocyte sedimentation rate (ESR) and levels of C-reactive protein (CRP), parathyroid hormone (PTH), and complement 3 (C3). ESR is a blood test that often reflects inflammation levels in the body. CRP is a marker of inflammation in the body. PTH is a natural hormone secreted by the parathyroid glands. Elevated PTH levels indicate a possible development of AS. C3 is an immune system protein. Higher than normal levels of C3 are associated with active AS. The acupuncture plus herbal medicine group significantly outperformed the drug control groups across all objective and subjective measures (p<0.05).
Design
Researchers (Wang et al.) used the following study design. A total of 108 patients were treated and evaluated in this study. The patients received treatment for ankylosing spondylitis and were randomly divided into three groups: an acupuncture plus herbal medicine group, an herbal medicine group, and a drug group, with 36 patients in each group. For the drug group patients, sulfasalazine was administered. The acupuncture plus herbal medicine group received acupuncture in addition to the identical herbal formula administered to the herbal medicine group.
The statistical breakdown for each randomized group was as follows. The acupuncture plus herbal medicine group was comprised of 28 males and 8 females. The average age in this group was 26.5 years. The average course of disease in this group was 3.2 years. The herbal medicine group was comprised of 30 males and 6 females. The average age in this group was 26.3 years. The average course of disease in this group was 3.6 years. The drug group was comprised of 27 males and 9 females. The average age in this group was 25.9 years. The average course of disease in this group was 3.9 years. There were no significant statistical differences in gender, age, and course of disease relevant to patient outcome measures for patients initially admitted to the study.
Treatment
For the drug group, patients received sulfasalazine tablets (0.25 g). For the first 5 days of treatment, the tablets were orally administered three times per day, one tablet each time. After 5 days, the tablets were given three times per day, two tablets each time. The treatment lasted for 60 consecutive days. The acupuncture plus herbal medicine group patients received acupuncture and Chinese herbal medicine. The primary acupoints used for the treatment group included the following:
- GV6 (Jizhong)
- Extra points (Huatuojiaji)
- BL23 (Shenshu)
- GV2 (Yaoshu)
- GB34 (Yanglingquan)
- Extra points (Ashi)
- GB33 (Yangguan)
- GV14 (Dazhui)
- GV9 (Zhiyang)
- GV8 (Jinsuo)
Treatment commenced with patients in a sitting position. After disinfection of the acupoint sites, a disposable filiform needle was inserted into each acupoint with a high needle entry speed. For Jizhong, Huatuojiaji, and Ashi points, the needles were inserted obliquely into each acupoint, with a maximum insertion of 1.5 cun. After a deqi sensation was obtained, the needles were manually stimulated with the Ping Bu Ping Xie (mild attenuating and tonifying) manipulation techniques.
For Yaoshu, Shenshu, and Yanglingquan, the needles were inserted perpendicularly to a depth of 1.0 cun. Then, the needles were manipulated with the xie (attenuating) technique with rotational speed reaching 80 r/min. For Yangguan, Dazhui, Zhiyang, and Jinsuo, the needles were inserted perpendicularly, reaching a maximum depth of 1.5 cun. After obtaining a deqi sensation, the needles were applied with the bu (tonifying) technique. The needles were retained for 20 minutes. One acupuncture session was conducted daily for 60 consecutive days. The Chinese herbal formula (modified Wuling decoction) used in the study included the following ingredients:
- Zhu Ling 10 g
- Ze Xie 15 g
- Niu Xi 10 g
- Qiang Huo 6 g
- Fu Ling 10 g
- Fang Feng 6 g
- Gui Zhi 7 g
A 300 ml decoction was made from fresh herbs each day, divided into two parts, and was administered in two servings, one in the morning and one at night, for a total of 60 consecutive days.
Laboratory and clinical data indicates that acupuncture plus herbal medicine is more effective for the treatment of ankylosing spondylitis than sulfasalazine. Acupuncture plus herbs improves symptoms and disease related biomarkers. Given the results of this investigation, additional research is warranted.
Reference:
Wang F, Wang MJ. Clinical Observation of Acupuncture Combined with Modified Wulingtang for the Treatment of Ankylosing Spondylitis, Journal of Basic Chinese Medicine [J], 2017,23(08):1135-1138.
